Introduction
One of the most fundamental terms in dentistry that is based on is ideal occlusion, and this forms the foundation upon which diagnosis, treatment planning, and restorative procedures will be based. In preclinical dental education, students are conditioned to think about occlusal principles at a tender age because they directly relate to how teeth work together in harmony during mastication, speech and mandibular movement. Knowledge of perfect occlusion enables future clinicians to fix teeth to allow them to preserve comfort, functioning, and the long-term oral health status.
In its simplistic form, occlusion is the association between the mandibular (lower) and maxillary (upper) teeth when they meet. The thorough knowledge of this relation is mandatory to prevent the occlusal disharmony, temporomandibular joint (TMJ) disorders, and restorative failures.
Gain knowledge of the general idea of Occlusion to have a broader basis of understanding.
Defining Ideal Occlusion
Ideal occlusion refers to a hypothetical arrangement of teeth whereby the top and bottom dental arches come into contact with one another in a stable, functional and aesthetically balanced relationship. Although there are differences in individuals in every case, ideal occlusion is used as an ideal in dental care both in education and clinical practice.
In ideal occlusion:
- They are properly aligned with teeth in the dental arches.
- There is a balance between cusp-fossa relationships.
- Biting forces are evenly decomposed.
- During the mandibular motion, there is no interference.
- The joints of the temporomandibular work symmetrically.
Dental students are educated to understand that ideal occlusion is not only a matter of fixed contact of the teeth, but also a matter of dynamic harmony when the teeth move.
To further build the conceptual base, students would tend to read doctrinal sources on occlusion like:
https://en.wikipedia.org/wiki/Occlusion (Wikipedia)
Centric Relation and Centric Occlusion
Centric Relation (CR)
One of the main concepts of the occlusion theory is the concept of centric relation. It is the location of the mandible as the condyles are in their most anterior-superior position in the glenoid fossa and the articular disc is in good play between them. Noteworthy, this posture does not depend on the contacts of teeth but rather is deemed as repeatable and stable.
Students are also taught that centric relation is a musculoskeletal position, rather than a tooth-determined position. It is extremely useful in the fields of prosthodontics and restorative dentistry.
Centric Occlusion (CO)
Centric occlusion (also referred to as maximal intercuspation) is the position of the teeth, or more precisely, the way of positioning the teeth, where they contact each other the most. In contrast to centric relation, this is a completely tooth-dependent position, which can vary depending on the alignment of the dentures, and their wear patterns.
One of the learning objectives in preclinical training is the realisation that CR and CO may or may not be equal. When the two do not fit correctly, occlusal discrepancies can be created which may result in functional disturbances.
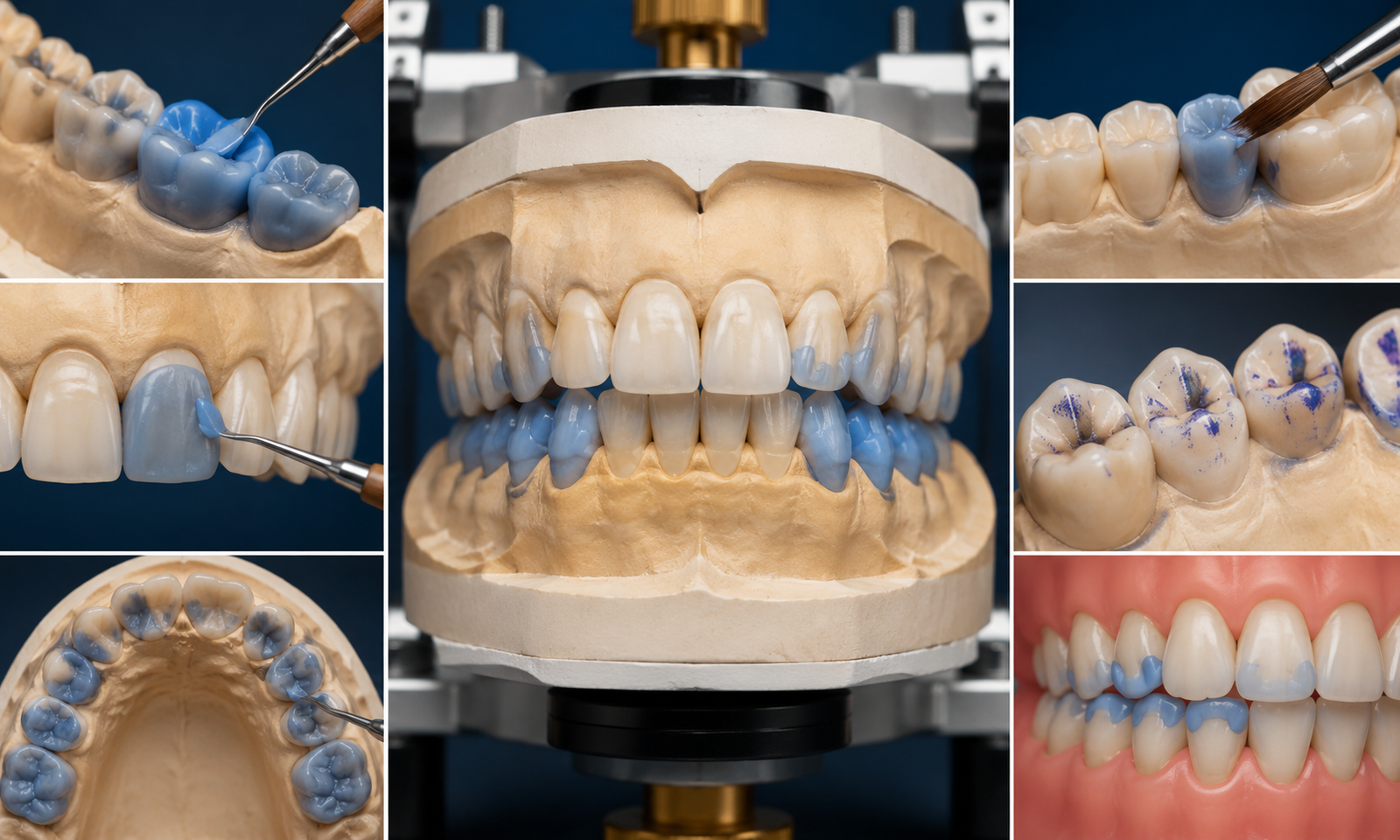
The Significance of the Intercuspation and Alignment.
A proper intercuspation is the way the cusps of the posterior teeth fit in the fossae and marginal ridges of the opposing teeth. This is one specific critical interlocking mechanism critical to efficient mastication and occlusal stability.
- Dental students are trained to observe:
- Cusp-fossa associations in the molars and premolars.
- Bend incisal advice in the front teeth.
- Symmetry and alignment of arches.
- Space at the contact points and spaces in the embrasure.
Intercuspation may cause uneven distribution of forces and this can lead to the wear, fracture or periodontal stress of teeth.
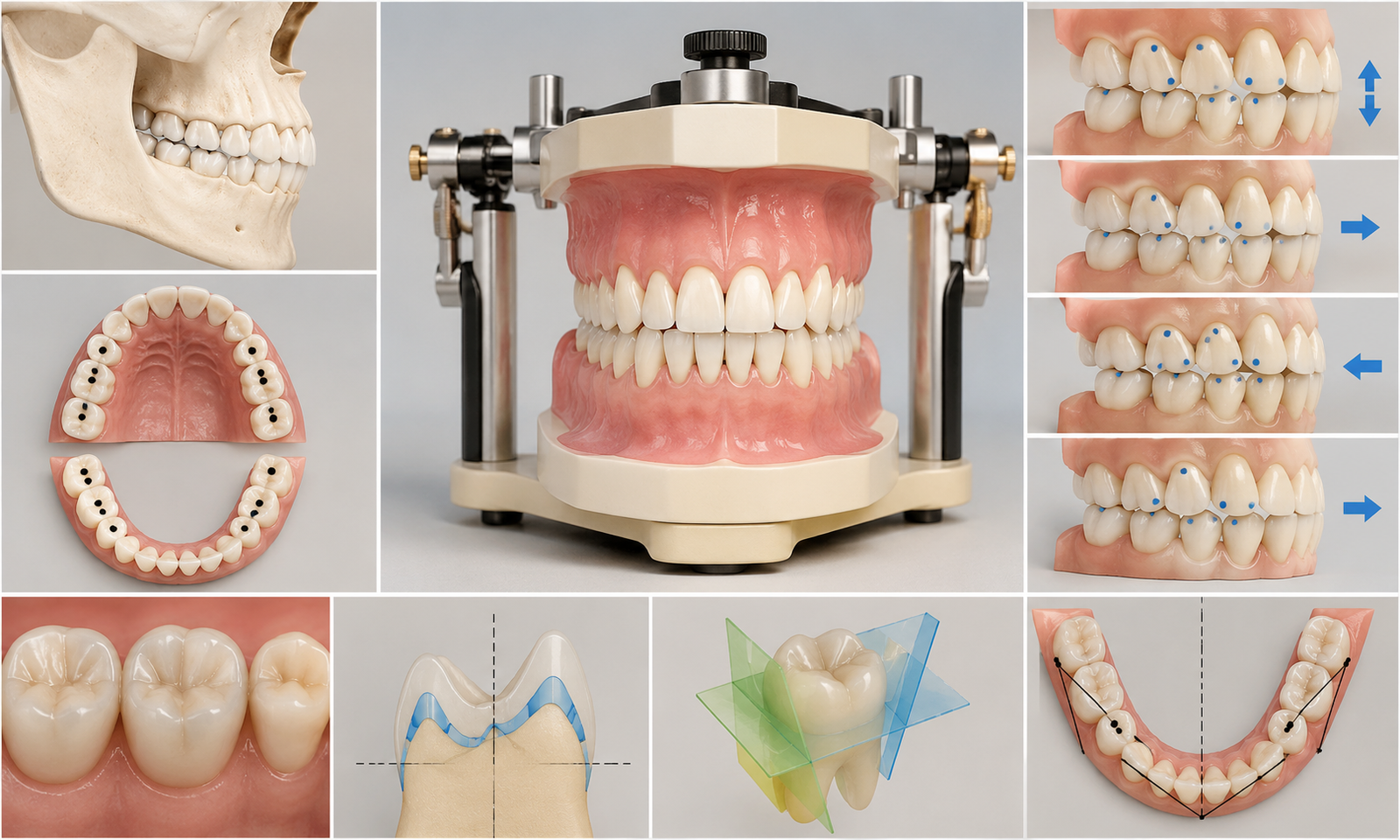
Mandible Movements Practical Movements.
The concepts of mandibular movement would help grasp the related art of occlusion. The mandible is not in one vertical movement, but it is a three-dimensional movement.
Key Movements Include:
- Opening movements and closing movements.
- Protrusion (forward movement)
- Retrusion (backward movement)
- Cross-town movement (lateral or side-to-side movement)
When such movements are involved the teeth have to guide the mandible without any interference. Here is where such ideas as canine direction and group action come into play.
During preclinical training, students can replicate these motions using articulators, which will enable them to visualize how the occlusal contacts play out in a dynamic manner.
Occlusal Stability and Purity.
Occlusal harmony means that there is a harmonious relationship between teeth, muscles and temporomandibular joints. When there is harmony, then the masticatory system works effectively without any strains and dysfunctions.
Students are taught that perfect occlusion is not just about the perfect symmetry but about the functional equivalence. Even the slight differences in occlusion may result in:
- Muscle fatigue
- TMJ discomfort
- Premature tooth wear
- Restorative failure
One of the objectives in the field of restorative and prosthetic dentistry is therefore the maintenance of occlusal stability.
A preclinical training in Occlusal Principles.
Preclinical dental education is essential in developing the knowledge base of a student on occlusion. Students spend much time on models, typodonts, and articulators to mimic real life occlusal situations.
The elements of the key training requirements entail:
- Tooth carving practice to learn about morphology.
- Putting dental casts on articulators.
- Documentation of the positions of centric relation.
- Simulating mandibular movements
- The examination of occlusional contacts and interferences.
This practical training enables the student to be space conscious concerning the interaction of the teeth in three dimensions.
The role of Articulators in Learning Occlusion.
Articulators are mechanical devices that replicate jaw movements. They play a vital role in starting an occlusion teaching because they enable students to learn dynamic relationships external to the mouth of the patient.
With articulators, students are able to:
- Visualize centric relation vs centric occlusion differences
- In movement evaluate the amount of contact made on the occlusives.
- Accurately place plan restorative restorations.
- Determine possible occlusion interferences.
This is a simulated learning that enhances clinical judgement prior to establishing the individual in contact with the patient.
Ideal Occlusion: Its clinical Relevance.
All the principles taught in preclinical occlusion are more applicable in clinical dentistry. Regardless of the restoration of a single tooth or creating a complete denture, the concept of occlusal harmony needs to be taken into account.
Applications Include:
- Restorative Dentistry: To make sure that the fillings and crowns do not interfere with the occlusion.
- Prosthodontics: Engineering dentures that have predictable bite interactions.
- Orthodontics: A good alignment and good functional bite.
- Endodontics: The prevention of post-treatment occlusal trauma.
Even technically perfect restorations can still fail because of non-observance of the principles of occlusivity.
Centric Relation Diagnostic Tool.
Of special concern when dealing with a high level of dental rehabilitation is centric relation. It offers a reproducible reference position which is not dependent on tooth wear or movement.
The dental students are taught to use centric relation as a base in:
- Full mouth rehabilitation.
- Occlusal adjustments
- Making of complete dentures.
- Treatment of severe malocclusion.
This concept in understanding will make sure that restorations are constructed on solid functional foundation.
Functional Occlusion vs Ideal Occlusion
One ought to identify ideal and functional occlusion. Although ideal occlusion is a theoretical concept, the functional occlusion is how the teeth of a patient really work in reality.
Not every patient shows textbook perfect occlusion, but the enormous amount of patients works flawlessly without any symptoms. Hence, dentists need to consider whether any clinical significance exists in the occurrence of occlusal deviations before taking action.
Learning Occlusion-Challenges.
The complexity of occlusion is three dimensional and the fact that anatomy, physiology and biomechanics have been integrated makes occlusion challenging to many dental students at the beginning.
Common challenges include:
- The pathways of mandibular motion.
- Understanding condylar dynamics
- Identifying occlusal interferences
- Differentiating CR and CO clinically
Nonetheless, they can be conquered with the help of the repeated practice with models and articulators.
Conclusion
Predicts of ideal occlusion make a pillar of preclinical dental education. With the acquisition of concepts like centric relation, centric occlusion, intercuspation, and mandibular movement, dental students have the basis to be successful in clinical practice.
The process of occlusion is not a fixed pattern of teeth but a dynamic process to which muscles, joints, and neuromuscular coordination process can be applied. It is through systematic training that the students learn to value this complexity and to implement it within restoration, prosthetic and orthodontic dentistry.
In the end, the good knowledge of the principles of occlusiveness also means that future dentists will learn to re-establish function, harmony and to retain the oral health accurately and confidently.