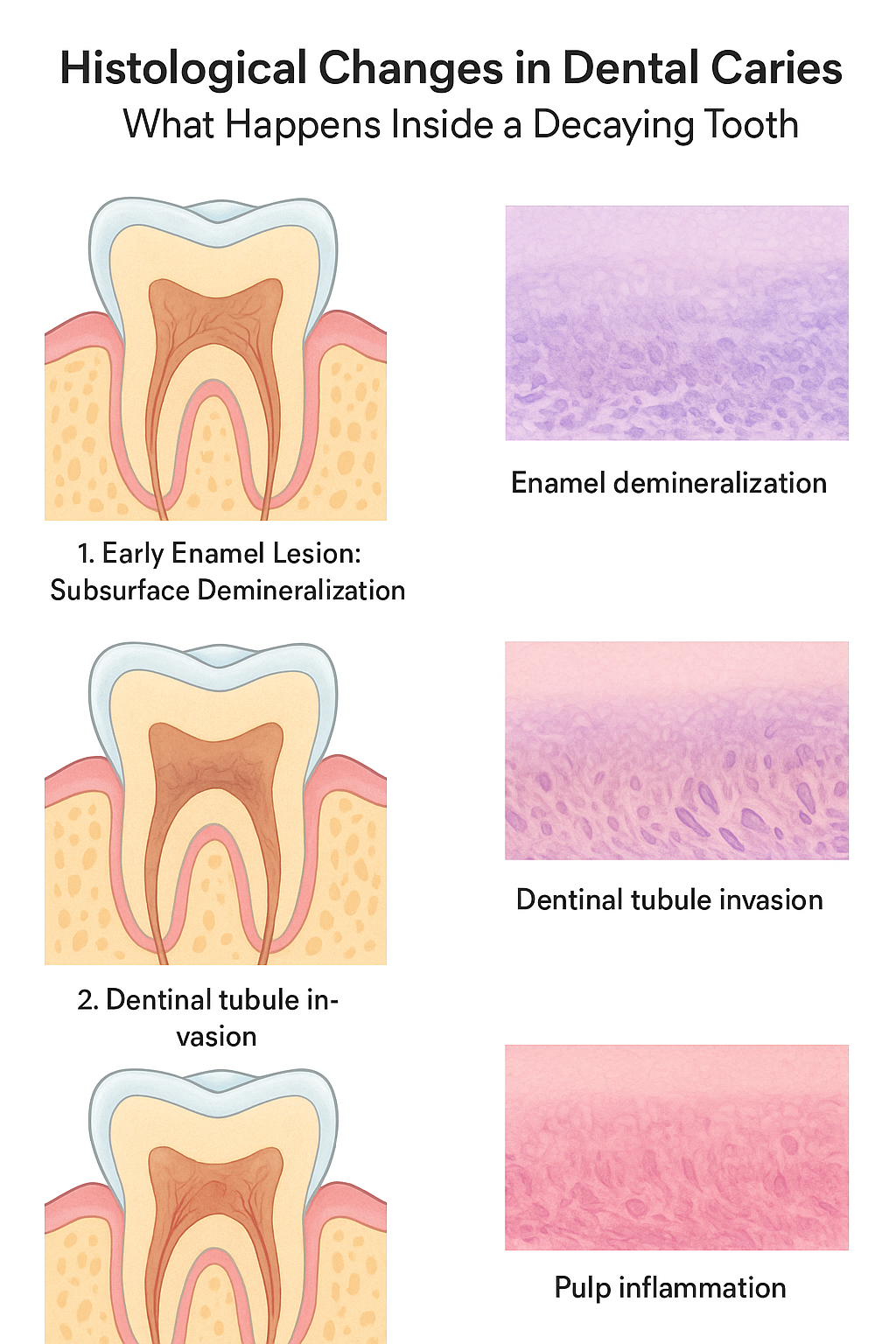
Dental caries is not just a superficial defect but it is a progressive histopathological process that changes the microscopic organization of enamel, dentin and pulp. These tissue-level changes are important to understand by clinicians, students, and patients who desire to understand the reason behind the irreversible damage by early intervention. The caries cause distinct microscopic impressions at every stage as it progresses inward through the enamel to the pulp and these impressions can be detected using the light microscope or the scanning electron microscope.
This article will take you through the histologic sequence of dental caries, beginning with the initial stages of early demineralization of the enamel to pulpal inflammation, and demonstrates exactly what occurs within a decaying tooth.
The Histopathology of Early Caries: Decay Starts Where
The caries of the teeth are initiated when the bacterial acids pass through enamel, dissolving the hydroxyapatite crystals. Alterations at this initial phase take place way before a cavity develops.
The First Stage Subsurface Enamel Demineralization
The first histological change is the formation of a lesion on the surface of a subsurface beneath an intact enamel. This is because the plaque organic acid diffuses inward destroying the enamel rods. Under the microscope, the lesion appears to include four different areas:
- Surface Zone
The relatively well-preserved layer (20-100 um) of the surface holds minerals as a result of the remineralizing effect of saliva.
- Body of the Lesion
The greatest part, which exhibited as much as 30 percent of mineral loss, with enamel prisms being dissolved and interprismatic spacing increased.
- Dark Zone
Gestures with punctured pores. It is a depiction of the regions experiencing mineral and demineralization cycles alternately.
- Translucent Zone
The lowest point that exhibits initial mineral dissolution, which can be observed because of a higher porosity.
Anchor link (as requested):
Get information on how to control enamel demineralization here:
It is difficult to control Enamel Demineralization.
At this stage, damage can be reversed when a lesion is observed at this phase and remineralization therapy is administered.
Structural Collapse and Cavitation When Enamel Break: Cavitation
When the erosion of the acid is more than remineralization by the enamel, microscopic voids form together and the cavitation occurs. Histologically:
- Enamel rods are lost in their orientation.
- Interprismatic substances are very soluble.
- The integrity of surfaces fails, leaving a visible hole.
- Bacteria infiltrate freely.
This represents the reversible-irreversible decay.
The Turning point in histological development to Dentin
During the invasion of the dentin by the dental caries, there is the encounter by a biologically active tissue which reacts dynamically to the invasion by the bacteria. Dentinal caries are more complicated histologically than enamel caries because of the existence of dentinal tubules, which are pathways to the pulp.
Zone 1- Subtransparent (Initial Demineralization) Dentin
This is a response that is done prior to the invasion by bacteria. Under the microscope:
- Minerals are lost through dentinal tubules and they enlarge.
- Peritubular dentin is worse than intertubular dentin which is degraded by acid.
- The collagen matrix starts to degenerate.
There are no bacteria at this point and remineralization can take place.
Zone 2 Transparent Dentin (Sclerotic Response)
In this case, the tooth is in self-defense.
Under the microscope, this layer appears:
- Tubular sclerosis: mineral deposition within tubules, either constricting or clogging the tubules.
- Growth of refractiveness under polarized light.
- Loss of permeability, retardation in bacterial progression.
This layer is not infected, although being demineralized, and can be maintained in the process of the conservative treatment.
Zone 3 – Turbid Dentin (Bacterial Invasion)
This is the most superficial layer that bacteria are found in.
Histological features:
- Several microorganisms in tubules.
- Loss of peritubular dentin, which will result in tubules that will be irregular and broadened.
- The collagen network collapses.
- Dentin is soft, and it is unable to be remineralized.
This is a layer that should be removed in cavity preparation.
Zone 4 Dentin Infection (Destruction and Necrosis)
Deep caries: This is the outermost layer.
- Heavily bacterial-laden.
- Totality of dentinal collagen.
- Amorphous debris is used in place of normal dentinal architecture.
- Permanently dead, and has to be dug out.
Dentinal Tubule Pathway: A Direct way to the Pulp
The dentinal tubules are directed towards the pulp, extending between the enamel and dentin junction (EDJ) to the pulp, and they get broader and more concentrated towards the pulp chamber. This constitution of the body implies:
- The further the caries move on, the more rapid are the bacteria.
- The higher density of tubules at the pulp increases the rate of inflammation.
- Microscopy reveals internal movement of streams of bacteria.
This structural fact indicates the reason why caries develop very fast in the area close to the pulp.
Pulpal Response: Microscopic Signs of Inflammation
Subsequently, the bacteria or their toxins penetrate the pulp, and the histological alterations are associated with the severity of the inflammation process.
Stage 1- Reversible Pulpitis (Mild Inflammation)
Under the microscope:
- Dilated blood vessels.
- Mild inflammatory infiltrate – preponderantly lymphocytes.
- Early disruption may be demonstrated in odontoblast layer.
- Minor periurethral edema.
At this point, pulpal health can be restored by the removal of caries and sealing of the dentin.
Stage 2 -Irreversible Pulpitis (Extensive Inflammation)
Histological signs are:
- Huge vascular congestions.
- Inflammation of neutrophils infiltrates.
- Micro-abscesses (small formations of abscess).
- Lack of or disorderly odontoblasts.
- Circulation impaired necrotic areas.
The effect of the elevated pulpal pressure in the rigid chamber is pain.
Stage 3 — Pulpal Necrosis
Total pulp dissolution ensues, which is defined by:
- Coagulative necrosis or liquefaction necrosis.
- Lack of usual cellular structure.
- The pulp chamber is colonized by bacteria.
- The intrusion into periapical tissue hence resulting in apical periodontitis.
The Importance of Early Detection – A Histological Examination
Knowledge about the microscopic pathogenesis of dental caries shows a number of critical clinical facts:
1. Lesions of the enamel are reversible
As early enamel demineralization does not affect the surface layer, remineralizing therapies are capable of restoring the surface layer.
2. Dentin infection cannot be reversed
Once the bacteria intrude into dentin, the effects that will be caused by the bacteria are irreparable since it is already permanent.
3. Involvement Pulpal involvement increases rapidly
Surface anatomy of tubules implies that deep caries may progress fast through the pulp causing it to be very important to detect early on.
4. Symptoms are preceded by changes in the microscopes.
Suffering typically manifests itself when the tissue has already been damaged significantly.
Conclusion
Dental caries is not a mere cosmetic display of surface discoloration but is a complicated histopathological condition that encompasses enamel, dentin and pulp. Since the first stages of demineralization of the initial enamel, the invasion by bacteria in the dentinal tubules, and subsequent pulpal necrosis, each of these stages is characterized by distinct microscopic alterations that define the prognosis and therapy.
Retaliation can be done at the stages when the tooth can still have a lot of chances to recover due to the early diagnosis. Bacterial invasion and pulpal necrosis have begun, and it is too late: there is no choice left but root canal treatment or extraction.
Knowledge of these sequential tissue changes allows clinicians and students to learn to treat caries as a biological process rather than as a clinical defect which is changing before the microscope.