Also referred to as the gums, the gingiva is not just the soft tissue that envelops our teeth but is also important in terms of keeping our mouth in excellent condition and in helping to guard the underlying periodontal structures. Knowledge of microscopic structure of healthy gingiva and changes in disease is essential in enabling clinicians to design effective periodontal treatments of diseases and avoid irreversible damages. We discuss the histological appearance of normal and diseased gums in this article with reference made to gingivitis and periodontitis.
Anatomy of Healthy Gingiva
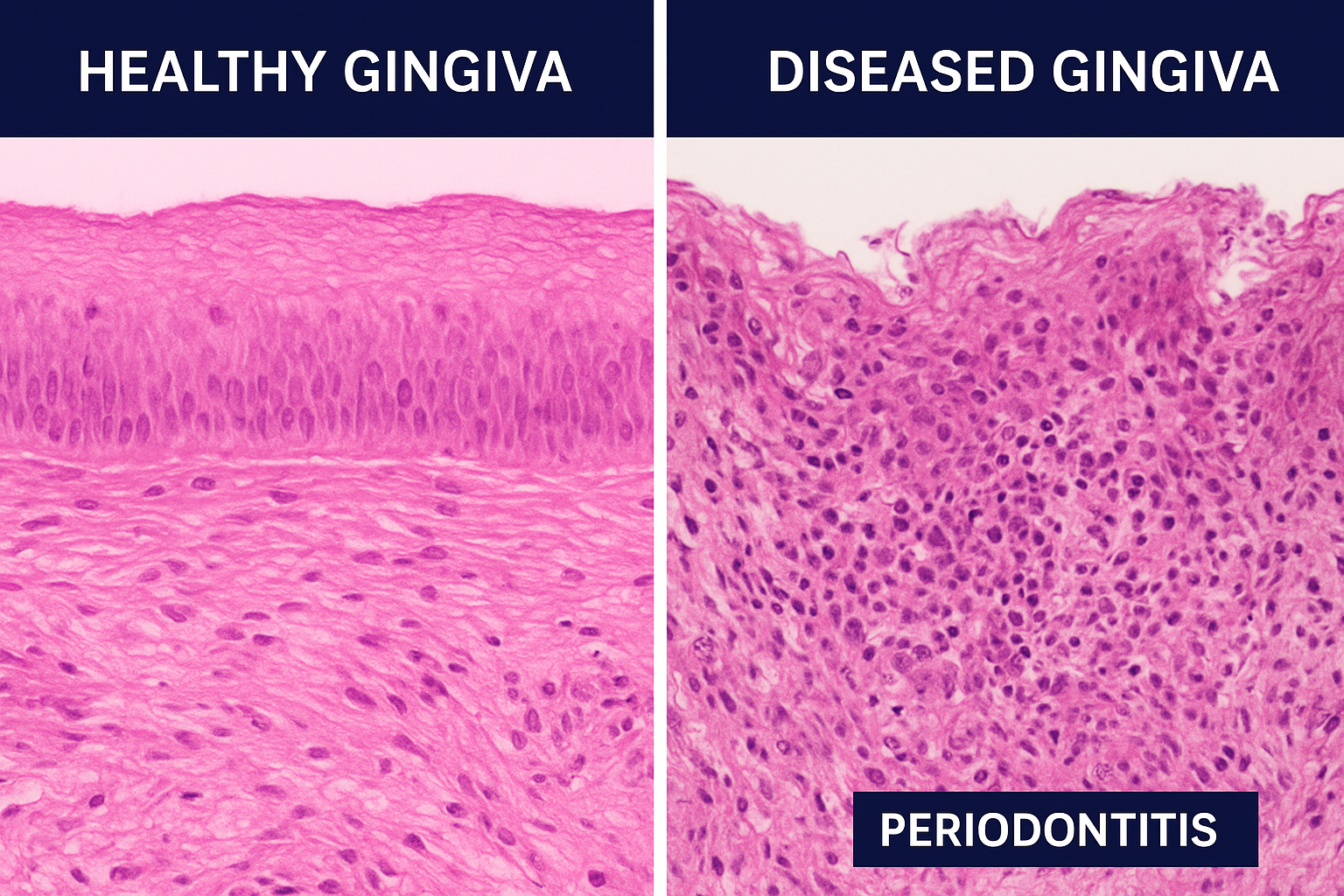
The microscopic level of the structure of healthy gingiva is highly organized and provides good resilience and defense against the invasion of microbes. It is composed of three major parts: epithelium, underlying connective tissue (lamina propria) and the junctional attachment to the tooth.
Epithelium
The lining of the gums is squamous keratinized epithelium of stratified type, that gives a strong resistance to mechanical forces and microbial invasion. Histologically it is subdivided into three areas:
- Oral epithelium: This is the surface that is in contact with the oral cavity and is keratinized especially in the attached gingiva. It is made up of various layers including the basal, spinous, granular and keratinized layer. The basal layer contains cells of the mitotically active cells which migrate to the surface to replace the lost cells.
- Sulcular epithelium: This is lining the gingival sulcus, and is non-keratinized and thinner than the oral epithelium. It is highly selective and permits the GCF that is composed of immune cells and antibodies to enter.
- Junctional epithelium: This is an epithelium that is attached to the cemento-enamel junction (CEJ). It has cells that are loosely packed with large intercellular spaces, which allows immunity to be monitored.
Lamina Propria
The connective tissue or lamina propria exists beneath the epithelium, and is mostly composed of dense collagen fibers, fibroblasts, blood vessels, and immune cells. The lamina propria gives the epithelium structural and functional support, provides nutrients, and supports immune reactions. The collagen fibers of healthy gingiva are well organized to give them tensile strength particularly in the attached gingiva which resists mechanical stress caused by mastication.
Immune Surveillance and Microvasculature
A good mobile capillary network, especially in the area of junctional epithelium, is an indication of healthy gingiva, which promotes metabolic activity and immune functions. Langerhans cells, lymphocytes and macrophages are resident immune cells that patrol the tissue and are ready to react to small challenges by microbes.
Histological Alterations of Gingivitis
The first stage of periodontal disease is called gingivitis and is defined by inflammation that is confined to the gingival tissues only without any damage to alveolar bone. Via the microscope, there are a number of differences between inflamed and healthy gingiva.
Epithelial Changes
- Hyperplasia: It is the thickening of the oral epithelium because of the additional layers of the epithelium in response to the chronic irritation of bacteria plaque.
- Keratinization: Keratinization can also be lost, becoming thin or irregular, which weakens the protective barrier of the tissue.
- Migration of Junctional Epithelia: Junctional epithelium is also anchored to the tooth in gingivitis but may exhibit some apical migration which when left unchecked will lead to periodontitis.
Connective Tissue Changes
- Edema and Collagen Breakdown: Due to the inflammatory mediators and prostaglandin and cytokines, vascular permeability is increased, leading to the development of edema. The collagen in the lamina propria is broken and disarranged.
- Inflammatory Cell Infiltration: Histologically, polymorphonuclear leukocytes (PMNs) lymphocytes and plasma cells are a dense infiltration of the connective tissue. The purpose of this immune response is to regulate the invasion of bacteria but causes the swelling and redness of the tissues that can be seen in the clinic.
- Microvascular Changes: Capillaries become dilated and the blood flow to the ganglionic tissue is increased resulting in the usual erythema of gingivitis.
Clinical Correlation
Such histological changes are the reason behind the typical symptoms of gingivitis which include red swollen gums which will bleed on probing. Although these changes occur, the alveolar bone has been spared hence gingivitis can be reversed by maintaining good oral health and using specific periodontal therapies.
Periodontitis: Changes at the histological level
Gingivitis can lead to periodontitis, which is a destructive disease, once uncontrolled, but is not limited to the gingiva, but can also damage periodontal ligament, alveolar bone and cementum. Periodontitis includes the microscopic characteristics which are more serious and signal tissue disintegration.
Epithelial Alterations
- Junctional Epithelium Migration and Pocket Formation: Junctional epithelium apical migration is one of the features of periodontitis. This can be historically followed as periodontal pockets which harbor bacterial biofilms and exacerbate inflammation.
- Ulceration and Necrosis: The chronic inflammation may cause some epithelial partial ulceration to expose the underlying connective tissue to bacterial invasion.
- Hyperplastic and Acanthotic Changes: Due to the continued irritation, the epithelium can have significant hyperplasia and acanthosis (thickening of the spinous layer).
Changes in Connective Tissues and Bones.
- Decalcification of Collagen Fibers: Collagen is substantially degraded in the lamina propria because of the release of matrix metalloproteinases (MMPs) by inflammatory cells. This undermines the gingivality and aids in extension of pockets.
- Chronic Inflammatory Cell Infiltrate: Lymphocytes, plasma cells, macrophages and neutrophils are persistently present in the connective tissue in a dense fashion.
- Osteoclastic Activity and Bone Loss: In periodontitis, inflammatory mediators activate osteoclasts which leads to the process of alveolar bone resorption–a characteristic of an advanced disease.
Vascular Changes
- Neovascularization: Inflammation in the long run causes the new capillary formation, which is often fragile, to underpin the metabolic requirements of infiltrating immune cells.
- Vascular Congestion: The preexisting capillaries look engorged and add to the redness and awareness to bleed that is found in the clinical picture.
Clinical Correlation
Periodontitis has histological changes which are associated with clinical manifestations including deep periodontal pocket, recession of the gum, tooth mobility and subsequent loss of tooth when unaddressed. Clinicians can use knowledge of these microscopic variations to determine the right type of periodontal therapy, whether it is scaling and root planing, use of antimicrobial therapy, or even surgery in extreme cases.
The Role of periodontal treatment planning with regards to histology
Clinicians cannot do without histological analysis of gingival tissue. It gives a microscopic validation of the severity of the disease which is at times underestimated in a clinical examination. Dentists are able to make a dentin intervention more targeted by assessing the integrity of epithelial cells, connective tissue arrangement, inflammatory infiltrates, and vascular alterations.
For instance:
- Early Gingivitis: Preventive measures, including professional cleaning and better oral health, can be recommended and justified by microscopic observation of mild inflammatory exudates and collagen destruction.
- Advanced Periodontitis: Junctional epithelium migration is observed to be accompanied by considerable connective tissue breakdown and osteoclastic activity, which justifies more aggressive treatment, which include periodontal surgery, bone grafting and guided tissue regeneration.
Histology is also useful in the monitoring of efficacy of treatment. A decrease in inflammatory cell infiltration and recovery of the connective tissue organization after intervention are signs of successful intervention.
Summary of Histological Differences
| Feature | Healthy Gingiva | Gingivitis | Periodontitis |
| Epithelium | Keratinized, organized | Hyperplastic, mild thinning of keratin layer | Hyperplastic, ulcerated, junctional epithelium migration |
| Connective Tissue | Dense collagen, minimal immune cells | Edematous, collagen disorganization, lymphocyte infiltration | Extensive collagen loss, dense inflammatory infiltrate, osteoclast activation |
| Vascularity | Fine capillary network | Dilated capillaries, increased blood flow | Neovascularization, vascular congestion, fragility |
| Clinical Outcome | Pink, firm gums | Red, swollen, bleeding | Pocket formation, gum recession, tooth mobility, potential tooth loss |
Conclusion
The microscopic analysis of the gingiva shows deep disparity between normal tissue and that of gingivitis or periodontitis. The epithelial structure of the healthy gingiva is highly organized, the collagenous connective tissue is dense, and the immune surveillance is under control, all of which bring resistance to the healthy gingiva. Conversely, gingivitis causes epithelial hyperplasia, destruction of connective tissue, inflammation by immune cells and vascular alterations. In periodontitis, these alterations are greater, and they usually lead to irreversible destruction of tissues and alveolar bone loss.
These histological changes do not simply represent a mere academic experiment. It provides clinicians with knowledge that can be applied in the planning and the implementation of focused periodontal treatments, including preventive procedures through advanced surgical procedures. Microscopic changes can be put under control at a very early stage leading to maintenance of periodontal health and loss of teeth is avoided.
With an understanding of the microscopic narrative of our gums, dental professionals are in a better position to overcome the hurdles of periodontal disease and deliver effective and evidence-based care to the patient.


