The human nervous system is a complicated system of neurons which regulate all the parts of our everyday functioning, including voluntary locomotion and sense perception. The most interesting of them are the cranial nerves, which are twelve pairs of nerves that directly appear out of the brain and brainstem. These nerves play a very important role in sensory functions and motor functions of the head and neck such as sight, hearing, taste, face expression and swallowing. The knowledge of cranial nerves is essential both in anatomy and clinical practice since the cranial nerves might be damaged, which will give a clear diagnostic hint in neurology.
The cranial nerves are identified by Roman numerals (I-XII) according to the sequence in which they develop out of the brain, the most anterior being the first. Every nerve possesses a distinct mixture of functions, either sensory, motor, or both (mixed), and has a certain anatomy of its ways to get to the target tissues. This paper will discuss the anatomy, functions, and areas of innervation of all the cranial nerves and serve as a complete resource to students, clinicians, and those who are interested in anatomy.
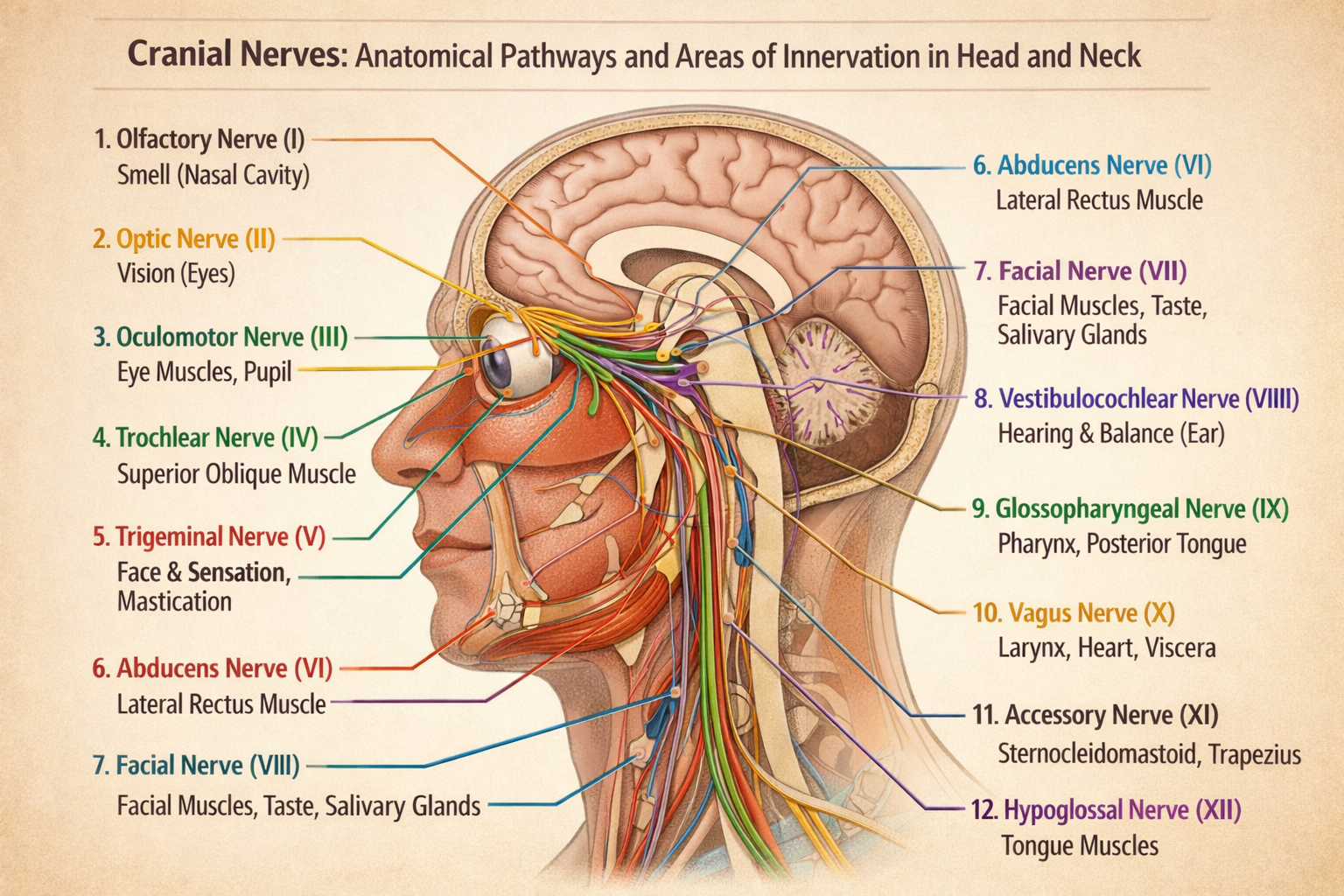
Overview of Cranial Nerves
The cranial nerves are symmetrical in form i.e. there is one nerve on both sides of the head. They are also unlike spinal nerves because they form as offshoots of the brain and not of the spinal cord. Generally, the cranial nerves may be classified according to their function:
- Sensory nerves: communicate the sensory organs to the brain (olfaction, sight, listening, balance, taste, etc.).
- Motor nerves: regulate the voluntary movements of the muscles, such as the ones involved in the movement of the eyes, facial expression, and swallowing.
- Mixed nerves: have sensory and motor activities.
To following shows an overview of the pathways of each nerve and its clinical implications.
- Olfactory Nerve (Cranial Nerve I)
Origin and Pathway:
Olfactory nerve develops as a result of olfactory receptor neurons found in the nasal epithelium. The passage of the fibers of this passes through the cribriform plate of the ethmoid bone to the olfactory bulb.
Function:
It is a sensory nerve, and is the mediator of the sense of smell (olfaction).
Areas of Innervation:
The olfactory nerve serves the nasal cavity mucous membrane, which allows the detection of the smell. Damage of such a nerve may lead to the loss of smell, or anosmia, an early sign of a disease such as traumatic brain injury or a neurodegenerative disease.
II. Optic Nerve (Cranial Nerve II)
Origin and Pathway:
The nerves of the eye are derivatives of ganglion cells. The fibers are united at the optic disc to create the optic nerve that goes through the optic canal into the cranial cavity. It partially decussates in the optic chiasm then proceeds to the lateral geniculate nucleus of the thalamus and the occipital visual cortex.
Function:
The optic nerve is all sensory and it transmits visual information.
Areas of Innervation:
It transmits light, color and movement data of the retina to the brain. Depending on the location of the injury, lesions can cause visual field defects including hemianopia.
III. The Oculomotor Nerve (Cranial Nerve III)
is found at the base of the brainstem associated with the spinal column of the skull.
Origin and Pathway:
The oculomotor nerve develops out of the midbrain at the superior colliculus level. It goes along the cavern sinuous and into the orbit through the superior orbital fissure.
Function:
It is mainly a motor nerve and controls the majority of extraocular muscles, the levator palpebrae superioris (eyelid lift), and the parasympathetic nerves restricting the pupil and the accommodation of the lens.
Areas of Innervation:
- There are superior, medial and inferior recti.
- Inferior oblique
- Levator palpebrae superioris.
- Sphincter pupillus (parasympathetic).
- Ciliary muscle (accommodation)
Oculomotor nerve damage manifests itself clinically in the form of ptosis (drooping eyelid), diplopia (ocular vision duplication), and dilation of the pupil.
IV. Trochlear Nerve (Cranial Nerve IV)
Origin and Pathway:
The trochlear nerve has its origin at the back of the midbrain, but it is the only nerve to decussate prior to leaving the brainstem. It goes along the superior orbital fissure to the eye.
Function:
It is an all motor nerve that regulates superior oblique muscle enabling the eye to gaze down and sideways.
Areas of Innervation:
- Superior oblique muscle
The damage of the trochlear nerve may also lead to vertical diplopia which is particularly apparent when reading or going up the stairs.
V. Trigeminal Nerve (Cranial Nerve V)
Origin and Pathway:
Trigeminal nerve is a branch of the pons that branches into three great ones:
- Ophthalmic (V1) – sensory
- Maxillary (V2) – sensory
- Mandibular (V3) -mixed (sensory and motor).
Function:
It is the primary facial sensory nerve as well as the anterior scalp nerve and motor nerve of the mastication muscles.
Areas of Innervation:
- Sensory: mouth, nose, the anterior part of the head, and cornea.
- Motor: masseter, temporal, mid and lateral pterygoid muscles.
Trigeminal neuralgia belongs to clinical relevance and comes as a form of severe facial pain in one or more of the branches.
VI. Abducens Nerve (Cranial Nerve VI)
Origin and Pathway:
The abducens nerve originates at the junction of the midbrain, goes through the cavernous sinu and to the orbit along superior orbital fissure.
Function:
It is a motor nerve that functions laterally on eye movement.
Areas of Innervation:
- Lateral rectus muscle
The outcome of damage is medial strabismus and horizontal diplopia because the damaged eye is not able to abduct.
VII. The Facial Nerve (Cranial Nerve VII)
Origin and Pathway:
The pons causes the facial nerve which exits the skull by the stylomastoid foramen through the internal acoustic meatus and it exits out of the skull.
Function:
It is an ambivalent nerve having various functions:
- Motor: facial expressive muscles.
- Sensation: anterior two-thirds of tongue.
- Parasympathetic: the sublingual, submandibular and lacrimal glands.
Areas of Innervation:
- Facial expression (orbicularis oculi, zygomaticus major) muscles.
- Tongue taste buds on the front.
- This is the salivary and lacrimal glands.
Bell palsy may be caused by facial nerve damage, which may result in weakness on one side of the face.
VIII. The Vestibulocochlear Nerve (Cranial Nerve VIII)
Origin and Pathway:
The vestibulocochlear nerve emerges out of the pons and medulla junction and enters the inner ear through the inner ear via the inner ear internal acoustic canal.
Function:
It is sensory and mediating hearing (cochlear branch) and balance (vestibular branch).
- Areas of Innervation:
- Cochlea (hearing)
- The equilibrium (vestibular apparatus).
Damage may lead to hearing impairment, vertigo and balance impairment.
IX. The Glossopharyngeal Nerve (Cranial Nerve IX)
Origin and Pathway:
The glossopharyngeal nerve develops out of the medulla, leaving the skull through the jugular foramen, and moving down onto the pharynx.
Function:
It is a mixed nerve:
- MotorStylopharyngeus muscle.
- Sensory: posterior one-third of the tongue (taste and general sensation)
- Parasympathetic: parotid gland.
Areas of Innervation:
- Pharynx and posterior tongue The pharynx and posterior tongue are inspected.
- Carotid body and sinus
- Difficulty in swallowing, loss of taste sensation are also considered as clinical significance on injury.
X. Vagus Nerve (Cranial Nerve X)
Origin and Pathway:
The vagus nerve is a derivative of the medulla, it leaves the skull through the jugular foramen, courses in the neck and thorax.
Function:
It is a crossed nerve having extensive activities:
- Motor: pharyngeal, laryngeal, soft palate 3.
- Sensation: viscera of thorax and abdomen, ear.
- Parasympathetic: gastrointestinal tract, lungs, heart.
Areas of Innervation:
- Pharyngeal/ laryngeal muscles (speech/ swallowing)
- Aboriginal and mesentery viscera.
Autonomic dysfunction, dysphagia, or hoarseness may be caused by vagus nerve injury.
XI. Accessory Nerve (Cranial Nerve XI)
Origin and Pathway:
This motor nerve develops out of the spinal accessory nucleus of the cervical spinal cord and medulla. It enters the skull through the foramen magnum and comes out through the jugular foramen.
Function:
It regulates muscles that take part in head and shoulder motion.
Areas of Innervation:
- Sternocleidomastoid
- Trapezius
The injury causes one to have weakness in rotation of the head and raising shoulders.
XII. Hypoglossal Nerve(Cranial Nerve XII)
Origin and Pathway:
The hypoglossal nerve forms out of the hypoglossal nucleus of the medulla, and leaves the skull through the hypoglossal canal.
Function:
It is a motor nerve which governs the movement of the tongue.
Areas of Innervation:
- Palatoglossus is an exception, but the tongue has intrinsic and extrinsic muscles.
Tongue deviation on the side of the lesion and speech and swallowing difficulties may also occur as a result of injury.
Clinical Relevance of Cranial Nerves
Clinical neurology and otolaryngology are centred on cranial nerves. A close observation can indicate minor neurological impairments that show the presence of lesions in certain nerves. For example:
- CNI can be a result of trauma or neurodegenerative disease.
- Optic neuritis or tumors may be heralded by changes to the vision (CNII).
- The facial asymmetry (CNVII) is an indication of Bell palsy or stroke.
- The presence of difficulty swallowing (CNIX, X) may be a sign of pathology of the brain stem.
The localization of the lesions, as well as planned interventions through anatomical pathways of these nerves, can be understood by clinicians.
Conclusion
The twelve cranial nerves are important pathways of sensory and motor fibres between the neck and head and the brain. Their various functions such as the capacity to experience smell and taste to the movement of their eyes and swallowing point to their implication in daily life and in clinical evaluation. The knowledge of the anatomy and physiology of the cranial nerves is not only beneficial in the field of understanding the neurology of the human being but it is the basis of diagnosing and treating neurological ailments.

